
Carotid Angioplasty and Stenting: A Modern Endovascular Approach
Understanding Asymptomatic Carotid Artery Disease
Carotid artery stenosis is a condition characterized by narrowing of the major arteries in the neck that deliver blood to the brain, most commonly due to atherosclerosis, or cholesterol plaque buildup within the arterial wall. In cases where the blockage becomes severe or stroke risk increases, carotid angioplasty and stenting may be considered as a minimally invasive treatment option to restore blood flow and reduce the likelihood of future cerebrovascular events.
While some patients experience warning signs such as a transient ischemic attack (TIA) or minor stroke, many individuals with significant carotid narrowing remain asymptomatic and feel completely normal.
Despite the absence of symptoms, high-grade carotid stenosis (≥70%) carries an increased long-term risk of ischemic stroke. Stroke remains a leading cause of death and disability worldwide. Preventing a first stroke in asymptomatic patients is therefore a major public health priority.
Modern management has evolved toward evidence-based endovascular therapy, particularly Carotid Angioplasty and Stenting (CAS), performed by experienced neurointerventional specialists.
What Is Carotid Angioplasty and Stenting?
Carotid Angioplasty and Stenting (CAS) is a minimally invasive, image-guided procedure designed to restore normal blood flow through a narrowed carotid artery.
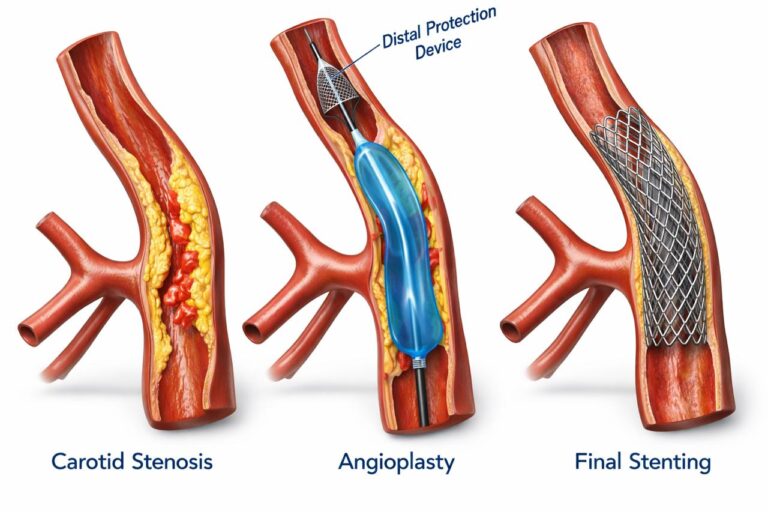
The procedure involves:
- Catheter navigation through a small puncture (wrist or groin access).
- Placement of an embolic protection device to capture debris.
- Balloon angioplasty to dilate the stenotic segment.
- Deployment of a self-expanding stent to scaffold the artery open.
Unlike open surgery, CAS avoids a neck incision, reduces cranial nerve injury risk, and typically allows faster recovery.
Scientific Evidence Supporting CAS
CREST
(Carotid Revascularization Endarterectomy vs Stenting Trial)
CREST enrolled over 2,500 patients with symptomatic and asymptomatic carotid stenosis. The trial demonstrated:
- Comparable long-term stroke prevention between CAS and surgery.
- Similar rates of the composite endpoint (stroke, myocardial infarction, or death).
- Slightly higher periprocedural stroke with CAS.
- Higher myocardial infarction rates with surgery.
Importantly, the 10-year follow-up confirmed durable equivalence in long-term stroke prevention, validating CAS as a scientifically sound alternative in properly selected patients.
Focus on Asymptomatic Disease: CREST-2
The management of asymptomatic carotid stenosis has entered a new era with CREST-2, one of the most important contemporary stroke-prevention trials.
CREST-2 consists of two parallel randomized trials comparing:
- Carotid stenting + intensive medical therapy
- Carotid endarterectomy + intensive medical therapy
- Versus intensive medical therapy alone
This design reflects a crucial scientific question:
In the era of modern statins, antiplatelets, blood pressure control, and lifestyle modification, which patients benefit most from revascularization?
CREST-2 emphasizes:
- Strict risk factor control
- High operator standards
- Modern stent technology
- Advanced embolic protection systems
The trial represents the most rigorous contemporary evaluation of asymptomatic carotid revascularization and reinforces the central role of endovascular expertise in preventive stroke care.
Modern Endovascular Advantages
Carotid stenting today is not the same as it was two decades ago. Advances include:
- Improved stent design (closed-cell, micromesh technology)
- Proximal and distal embolic protection devices
- Radial artery access for enhanced patient comfort
- Real-time neuro-monitoring
- High-definition vascular imaging
In experienced centers, contemporary stroke/death rates for asymptomatic CAS are consistently below 3%, meeting international safety benchmarks.
The endovascular approach offers:
- No neck incision
- Lower cranial nerve injury risk
- Minimal hospital stay
- Rapid return to normal activity
Who Should Consider Carotid Stenting?
Patients with:
- High-grade asymptomatic carotid stenosis (≥70%)
- Long life expectancy
- High surgical risk or preference for minimally invasive therapy
- Favorable vascular anatomy
Careful patient selection is essential. Duplex ultrasound, CT angiography, and multidisciplinary evaluation guide decision-making.
Stroke Prevention in the Modern Era
The future of carotid disease management lies in:
- Personalized risk stratification
- Plaque imaging (vulnerability assessment)
- Precision endovascular techniques
- Intensive medical therapy integration
Carotid Angioplasty and Stenting represents the evolution of stroke prevention toward minimally invasive, data-driven care.
Key Takeaway
Carotid Angioplasty and Stenting (CAS) is a scientifically validated, minimally invasive treatment for carotid artery stenosis. Supported by robust long-term data from CREST and strengthened by ongoing evidence from CREST-2, CAS plays a central role in modern stroke prevention—especially in asymptomatic carotid disease.
Early detection, expert evaluation, and advanced endovascular treatment can prevent devastating stroke before it happens.
Stroke prevention is not just treatment—it is proactive protection of the brain.
- 022-61305089
- drnishant@stroketreatment.in
- nishantaditya@yahoo.com