Intracranial Angioplasty and Stenting for Severe ICAD
For selected patients with severe intracranial atherosclerotic disease (ICAD), intracranial angioplasty and stenting have emerged as a precision-based treatment strategy designed to reduce recurrent stroke risk and restore cerebral blood flow.
Intracranial atherosclerotic disease (ICAD) is a condition in which cholesterol plaque builds up inside the arteries within the brain. Unlike carotid disease in the neck, ICAD affects vessels such as the middle cerebral artery (MCA), the intracranial internal carotid artery (ICA), the vertebral artery, and the basilar artery.
ICAD accounts for approximately 8–10% of ischemic strokes in Western populations and up to 30–50% in Asian populations, making it a major global stroke burden. Patients with severe intracranial stenosis (70–99%) face a particularly high risk of recurrent stroke, especially within the first year after a symptomatic event.
Despite aggressive medical therapy (dual antiplatelets, high-intensity statins, blood pressure control), recurrent stroke risk in high-grade ICAD can approach 12–20% within one year in selected high-risk subgroups. This unmet clinical need has driven the evolution of intracranial angioplasty and stenting as a refined, carefully selected endovascular strategy.
What Is Intracranial Angioplasty and Stenting?
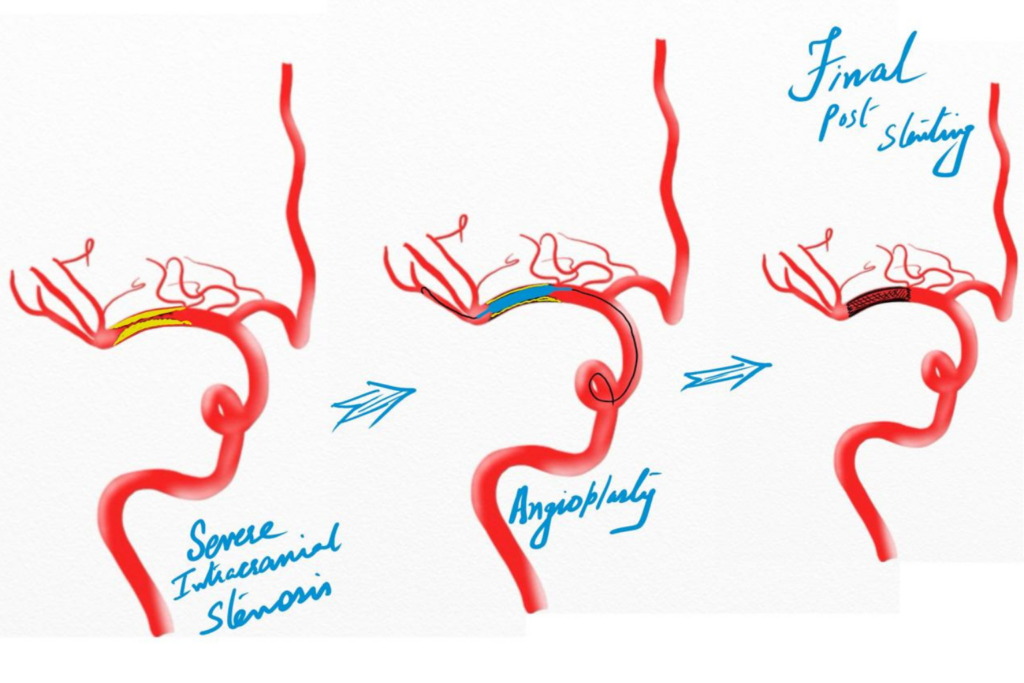
Intracranial angioplasty and stenting is a minimally invasive procedure performed through a small arterial puncture (usually radial or femoral access). Under high-resolution fluoroscopic guidance:
- A microcatheter is navigated to the narrowed brain artery.
- A balloon is gently inflated to dilate the stenotic segment.
- In selected cases, a self-expanding intracranial stent is deployed to maintain vessel patency.
Modern techniques emphasize:
- Careful lesion selection
- Undersized balloon angioplasty
- Controlled inflation strategies
- Experienced neurointerventional expertise
The goal is to restore cerebral blood flow and prevent recurrent ischemic stroke.
Modern Clinical Evidence Supporting Intracranial Stenting
While early broad-application trials showed cautionary signals, contemporary evidence highlights that patient selection, timing, and operator experience are critical determinants of safety and efficacy.
WEAVE
The WEAVE trial evaluated strictly on-label use of the Wingspan intracranial stent system in carefully selected patients with symptomatic high-grade stenosis.
Key findings:
- Periprocedural stroke and death rate: 2.6%
- Significantly lower complication rates compared to earlier experiences
- Demonstrated safety when strict criteria and experienced operators were applied
This study marked a turning point by showing that intracranial stenting, when properly selected, can be performed safely.
WOVEN
WOVEN, the one-year follow-up of WEAVE patients, demonstrated:
- Sustained stroke prevention benefits
- Acceptable long-term outcomes
- Reinforcement of strict patient selection principles
Together, WEAVE and WOVEN reframed intracranial stenting as a precision-based intervention rather than a blanket treatment approach.
Who Benefits Most?
Current evidence suggests intracranial angioplasty and stenting may be considered in patients with:
- Symptomatic 70–99% intracranial stenosis
- Recurrent stroke despite optimized medical therapy
- Hemodynamic compromise demonstrated on imaging
- High-risk posterior circulation stenosis (e.g., basilar artery)
In these subgroups, recurrent stroke risk without intervention remains clinically significant.
Advances in Endovascular Technology
Modern intracranial intervention benefits from:
- Flexible, low-profile stent systems
- Enhanced deliverability through tortuous anatomy
- High-resolution biplane angiography
- Improved antiplatelet monitoring
- Radial artery access options
These technological improvements have dramatically reduced complication rates in experienced centers.
Safety and Long-Term Outcomes
When performed under strict indications:
- Periprocedural complication rates are often below 3–5% in contemporary registries.
- Restenosis rates are manageable with follow-up imaging.
- Carefully selected patients demonstrate a meaningful reduction in recurrent stroke risk.
Importantly, intracranial stenting is not first-line therapy for all ICAD patients. Aggressive medical management remains foundational. Endovascular therapy is reserved for high-risk, medically refractory cases.
The Future of Intracranial Revascularization
Ongoing research is focusing on:
- Drug-eluting intracranial stents
- Advanced plaque characterization imaging
- Hemodynamic flow assessment tools
- AI-based stroke recurrence prediction
The field is evolving toward individualized cerebrovascular precision medicine.
Key Takeaway
Intracranial angioplasty and stenting represent a highly specialized, minimally invasive treatment option for carefully selected patients with severe, symptomatic intracranial arterial stenosis.
Modern studies such as WEAVE and WOVEN demonstrate that, when performed under strict criteria by experienced neurointerventional teams, intracranial stenting can be safe and effective.
For patients suffering recurrent stroke despite optimal medical therapy, advanced endovascular revascularization offers hope, precision, and protection of vital brain function. Stroke prevention in complex intracranial disease demands expertise, technology, and thoughtful patient selection—the pillars of modern neurointerventional practice.
FAQs
How does intracranial angioplasty and stenting work?
A microcatheter is guided to the narrowed artery, a balloon is inflated to widen the vessel, and in selected cases, a self-expanding stent is placed to maintain long-term patency.
Is intracranial angioplasty and stenting safe?
When performed by experienced neurointerventional specialists under strict patient selection criteria, modern studies show periprocedural complication rates typically below 3–5%.
What are the risks of intracranial angioplasty and stenting?
Potential risks include stroke, vessel injury, bleeding, in-stent restenosis, and reaction to contrast. Careful case selection significantly reduces these risks.
How long does the intracranial angioplasty and stenting procedure take?
The procedure typically takes 1–3 hours, depending on vascular anatomy and lesion complexity.
What is the recovery time after intracranial angioplasty and stenting?
Most patients stay in the hospital for monitoring for 1–2 days and resume normal activities within a week, depending on individual recovery.