
The human brain is serviced by a vast network of blood vessels, organized with military precision. However, in rare cases, a structural “short circuit” known as an Arteriovenous Malformation (AVM) disrupts this flow. Understanding this condition is the first step toward preventing a life-threatening crisis.
When dealing with a vascular anomaly of this complexity, the expertise of a specialized brain stroke physician and the advanced infrastructure of a high-volume brain stroke centre are your most powerful allies.
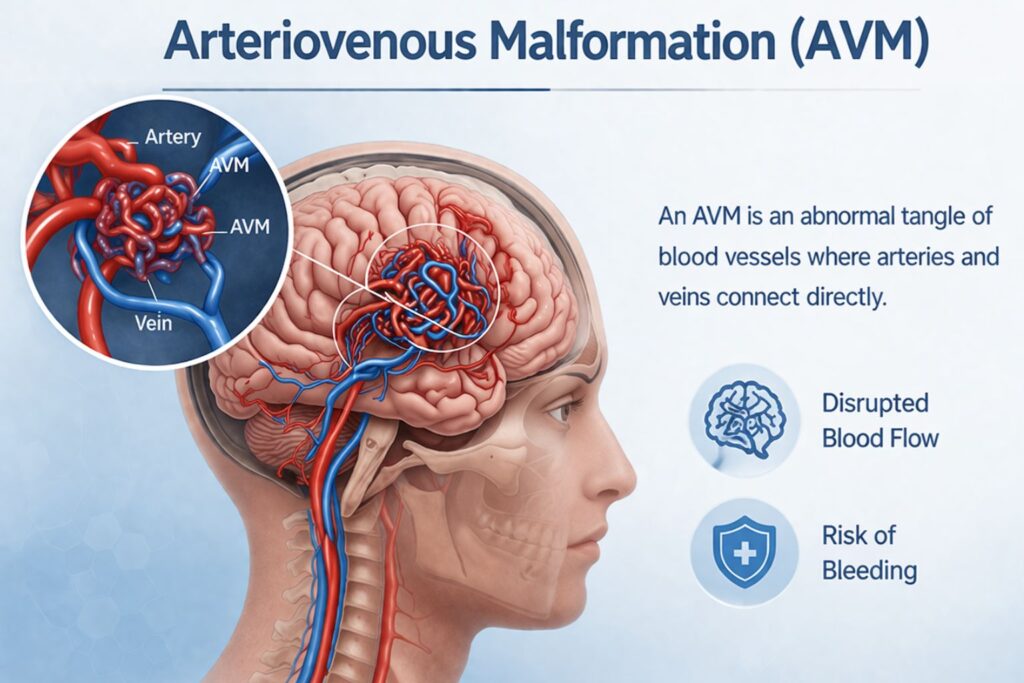
What is an Arteriovenous Malformation (AVM)?
In a healthy circulatory system, high-pressure arteries carry oxygenated blood to the brain. This blood then enters tiny, thin-walled capillaries that slow down the flow, allowing oxygen to reach brain cells. Finally, the blood drains into low-pressure veins to return to the heart.
An AVM is a tangled “nest” of blood vessels (called a nidus) where arteries connect directly to veins, completely bypassing the capillary bed.
The Danger of the “Short Circuit”
Because there are no capillaries to dampen the pressure, high-velocity arterial blood slams directly into the fragile veins. Over time, these veins can:
- Stretch and dilate (forming aneurysms).
- Leak or rupture, causing a hemorrhagic stroke.
- “Steal” blood from surrounding healthy brain tissue, leading to neurological decline.
Recognising the Symptoms: When to Seek a Stroke Centre
Many people live with an AVM for years without knowing it. Symptoms typically emerge between the ages of 10 and 40.
Common Warning Signs:
- Seizures: Often the very first indication of an underlying vascular issue.
- Sudden, Intense Headaches: Often localized to one side of the head.
- Neurological Deficits: Muscle weakness, numbness, or paralysis in one part of the body.
- Pulsatile Tinnitus: A rhythmic “whooshing” sound in the ear, caused by high-pressure blood rushing through the AVM.
- Vision Problems: Sudden blurriness or loss of peripheral vision.
Precision Diagnosis at a Brain Stroke Centre
Standard imaging often misses the intricacies of an AVM. A dedicated brain stroke physician utilizes specialized tools to map the nidus:
- MRI & MRA: To identify the AVM’s exact location and its relationship to “eloquent” brain areas (speech, movement).
- CT Angiography (CTA): Provides a 3D view of the vessel structure.
- Digital Subtraction Angiography (DSA): The “Gold Standard” test. A thin catheter is threaded to the brain, and dye is injected to capture the high-speed flow of the AVM in real-time.
Treatment Pathways: The Multidisciplinary Approach
At a top-tier stroke treatment centre is never “one size fits all.” A team of specialists—including neurosurgeons and interventional neuroradiologists—collaborate on a custom plan.
1. Endovascular Embolization (Minimally Invasive)
The physician navigates a microcatheter into the AVM nidus and injects a “liquid embolic agent” (a medical-grade glue). This plugs the abnormal vessels, reducing the risk of bleeding or preparing the AVM for safer surgical removal.
2. Microsurgical Resection
A neurosurgeon performs a craniotomy to carefully disconnect the AVM from its feeding arteries and draining veins. Once the tangle is removed, the risk of future hemorrhage is eliminated.
3. Stereotactic Radiosurgery (Gamma Knife)
For AVMs located deep in the brain where surgery is too risky, focused radiation beams are used. Over 1 to 3 years, the radiation causes the AVM vessels to slowly thicken and close off.
Why the Facility Matters
Successfully treating an AVM requires more than just a surgeon; it requires a stroke centre equipped with:
- Hybrid Operating Rooms: Where surgical and catheter-based treatments can happen in one session.
- Advanced ICU Support: For precise blood pressure management post-procedure.
- Rehabilitative Experts: To help patients regain function if a bleed has already occurred.
FAQs
Can an AVM “grow back” after it is removed?
If a brain stroke physician confirms total removal via a post-op angiogram, the recurrence rate is extremely low. Total surgical removal is considered a permanent cure.
Are all AVMs treated immediately upon discovery?
Not always. If an AVM is in a very high-risk area and hasn’t bled, a physician might choose “watchful waiting.” However, most are treated to prevent the catastrophic risk of a future rupture.
What is the recovery time for embolization?
Since it is minimally invasive, most patients stay in the stroke centre for 24–48 hours for observation and return to light activities within a week.
How does an AVM cause a stroke?
An AVM causes a hemorrhagic stroke when the high-pressure blood causes a vessel to burst, spilling blood into the brain tissue and starving cells of oxygen.
Is exercise safe if I have a known AVM?
Patients with known AVMs are usually advised to avoid heavy lifting or high-intensity strain that significantly spikes blood pressure until the AVM is treated.
Conclusion
An arteriovenous malformation is a silent but serious condition. However, with the rapid advancement of endovascular tools and microsurgery, the prognosis for AVM patients has never been better. Early diagnosis by an experienced brain stroke physician at a specialized brain stroke centre is the key to a long, healthy life.