
When a neurological emergency strikes, most people immediately think of a traditional stroke. However, there is a specialized area of medicine focused on the brain’s “drainage system”—the dural venous sinuses. When these pathways are compromised, it takes a specialized brain stroke physician and a high-tech stroke centre to prevent permanent damage.
Understanding the Brain’s Drainage System
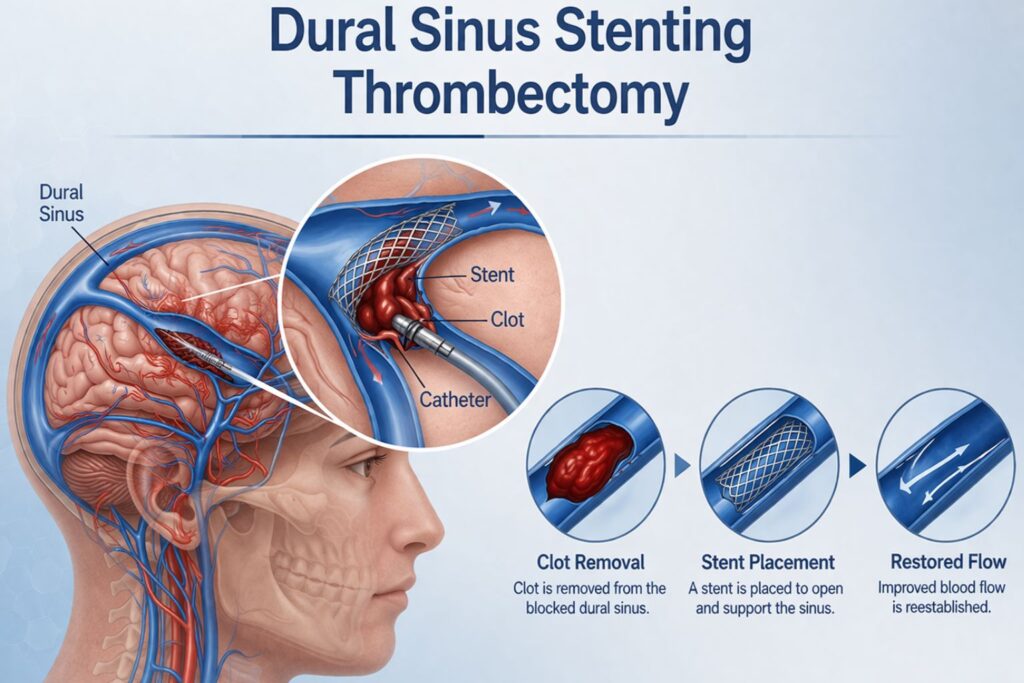
The dural sinuses are channels that collect deoxygenated blood and cerebrospinal fluid (CSF) to carry them away from the brain. If these channels become blocked by a clot (Thrombosis) or narrowed by pressure (Stenosis), the “plumbing” backs up. This leads to increased intracranial pressure, which can cause strokes, vision loss, or severe hemorrhaging.
1. Dural Sinus Thrombectomy: The Emergency Rescue
Cerebral Venous Sinus Thrombosis (CVST) is a life-threatening condition where a blood clot forms in these sinuses. Unlike an arterial stroke, CVST often affects younger adults and can be triggered by dehydration, pregnancy, or clotting disorders.
When is it performed?
While blood thinners are the first line of defense, a brain stroke physician will pivot to a mechanical thrombectomy if the patient:
- Develops worsening neurological deficits.
- Experiences frequent seizures or coma.
- Shows signs of a brain bleed (hemorrhage).
The Procedure
Working within a specialized stroke centre, the physician uses a minimally invasive approach. They thread a catheter from the groin or wrist directly into the brain’s venous system. Using a combination of aspiration (suction) and stent-retrievers (mesh cages), the clot is physically captured and removed, instantly restoring the brain’s ability to drain blood.
2. Dural Sinus Stenting: Precision for Chronic Pressure
While thrombectomy handles sudden clots, Dural Sinus Stenting is the primary treatment for Venous Sinus Stenosis. This narrowing is the leading structural cause of Idiopathic Intracranial Hypertension (IIH)—a condition where brain pressure rises so high it mimics a tumor.
Warning Signs of Stenosis:
- Pulsatile Tinnitus: A rhythmic “whooshing” sound in your ears that matches your pulse.
- Papilledema: Swelling of the optic nerve that causes blurred vision or “graying out.”
- Intense Headaches: Constant pressure that is often worse in the morning.
The Procedure
At a brain stroke centre, the physician places a small, self-expanding metal stent across the narrowed segment of the vein. This “props open” the channel, allowing blood to flow freely and immediately dropping the internal pressure. For many, the “whooshing” sound in their ears stops the moment the stent is deployed.
Why the Facility and Physician Matter
These procedures are highly technical and require a multidisciplinary approach only found at a dedicated brain stroke centre.
- Expert Diagnosis: A specialized brain stroke physician uses advanced MRV and CTV imaging to see “venous” issues that standard CT scans often miss.
- 24/7 Intervention: Venous strokes don’t keep business hours. A top-tier stroke centre has neuro-interventionalists on standby 24/7.
- Integrated Recovery: Post-procedure care involves managing blood pressure and specific anti-clotting medications to ensure the stent remains open.
Recovery: What to Expect
Because these are “endovascular” (inside-the-vessel) procedures, there is no large incision on the head.
- Observation: Most patients stay in the hospital for 1–2 days for monitoring.
- Immediate Relief: Symptoms like vision blurring and pulsatile tinnitus often improve within hours.
- Long-term Care: Patients typically take blood-thinning or antiplatelet medication for several months to prevent future clots.
Conclusion
If you are experiencing symptoms like rhythmic ear noises or unexplained vision changes, do not wait. Early consultation with a brain stroke physician at a specialized brain stroke centre can be the difference between a full recovery and permanent disability. Every second counts when it comes to the brain’s “plumbing
FAQs
1. How long does a dural sinus stenting or thrombectomy procedure take?
Typically, these minimally invasive procedures take between 1 and 3 hours, depending on the complexity of the clot or the degree of narrowing in the sinus.
2. Is dural sinus stenting a permanent solution?
Yes, the stent is designed to stay in the vein permanently. It acts as a scaffold to keep the vessel open, and over time, the body’s natural vessel lining grows over the mesh.
3. What is the success rate of mechanical thrombectomy for CVST?
When performed at a high-volume stroke centre, success rates for restoring blood flow (recanalization) are very high, often exceeding 80–90%, significantly improving recovery outcomes compared to medication alone.
4. Will I need to take blood thinners after getting a stent?
Yes. Most patients are prescribed antiplatelet medications (like Aspirin or Clopidogrel) for several months to a year to prevent new clots from forming on the stent surface.
5. Can these procedures prevent permanent vision loss?
Absolutely. For patients with IIH or stenosis, stenting reduces the pressure on the optic nerve (papilledema). If caught early by a brain stroke physician, this can stop or even reverse vision deterioration.